The simulation revolution
Developed on the Gold Coast, translational simulation is improving healthcare internationally


The simulation revolution
Developed on the Gold Coast, translational simulation is improving healthcare internationally
Having worked at the coal face of emergency departments for 25 years, Bond University Professor of Emergency Medicine Victoria Brazil knows firsthand the challenges of ineffective systems. She has turned frustration into action, developing a method for improving healthcare quality, coined ‘translational simulation’. Today, it is used internationally to help build hospitals and services that function well, improving outcomes for patients, doctors and allied health professionals.
A new partnership between Bond and Norwegian firm Laerdal is taking it into the future, using artificial intelligence to enhance access and outputs.
Translation simulation explained
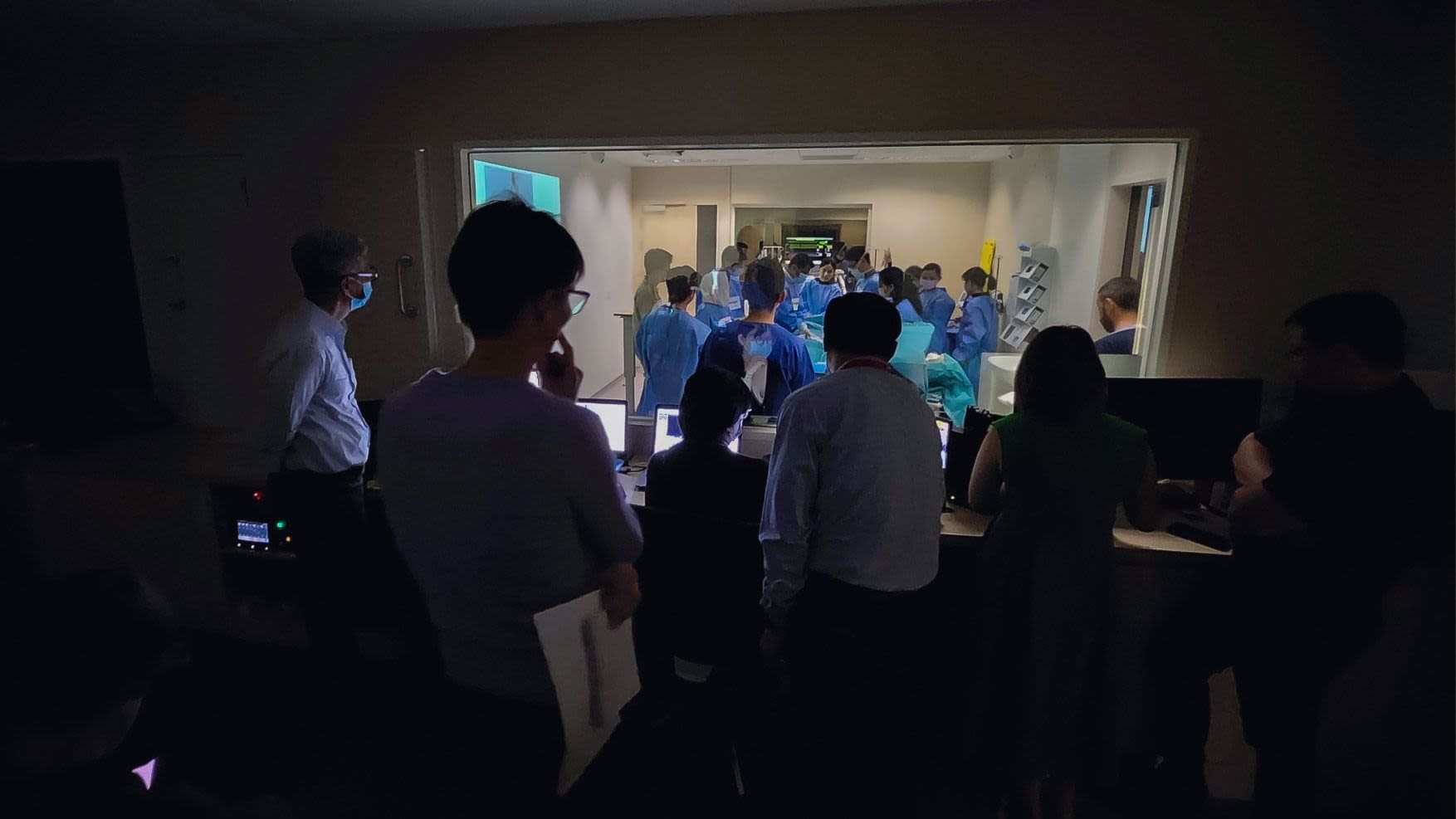
Put simply, translational simulation uses simulation exercises to improve quality and safety in healthcare. Unlike traditional medical simulations, it does not focus on education but rather exploring, and enhancing, the systems in which health professionals work.
“Translational simulation assumes practitioners already know what they’re doing and asks, what do you need from the system to help you?” Professor Brazil says.
It could be the design of a physical space, like the triage area of an emergency department, or to improve processes and workflows. Professor Brazil says the simulations often use actors, mannequins or cardboard cut-outs to ensure environments and systems are user-centred, often before departments are operational.
“It can be used to improve processes like getting patients through their journey faster, which is particularly important in time critical scenarios like stroke, heart attack or trauma,” she explains.
“We're asking practitioners, what do you need to smooth the process? Should we have different call systems? Should we have checklists to help you get ready? Should we have parallel processing, so we are not slowing down the patient journey?”
The origins of translational simulation
Professor Brazil says her own clinical background sparked her desire to explore the bigger picture of how systems can be improved to resolve the frustrations that can impact medical staff on a day-to-day basis.
“As emergency physicians, we become very attuned to systems in hospitals. Yes, we work one-on-one with patients, but we are often at the nexus of systems that either work for us or don't,” she says.
“The accelerator for me was the building of the new Gold Coast University Hospital. I started working at Bond at the same time as the hospital, so I was working in both education and the health service.”
Focused on meeting high safety and quality goals at the new hospital, Professor Brazil developed protocols and procedures for new departments including the trauma service, maternity service, and the Children’s Critical Care unit.
“There were very enthusiastic clinicians who wanted to get it right, so simulation was a natural way for us to test and refine,” she says.
At the same time, others were using simulations in the clinical environment, leading to debate among practitioners. Professor Brazil published an article in 2017 addressing the discussions, where she first coined the phrase translational simulation. It has since been cited more than 120 times.
“People were arguing about what was better, simulations ‘in situ’ or in simulation labs, and I said, ‘it's not about where we do it, it's about why we do it’,” she says.


The real impact on patients, doctors and allied health professionals
Time based targets are an obvious benchmark and, Professor Brazil says, relatively easy to achieve with effective simulations.
“One of my first was with the Royal Brisbane and Women’s Hospital back in 2011. After six months of simulations focusing on improving processes, we halved the time it took patients to get from the emergency department to the cath lab to diagnose and treat heart conditions,” she says.
“That’s a dramatic improvement, but there are many benefits you can't quantify that are just as meaningful.”
She points to a project involving an electroconvulsive therapy unit, where simulations involving actors uncovered those in the waiting area could hear activity in the treatment room, which could have been traumatising to real life patients.
“We shifted the waiting area to a different part of the building. You can’t put a statistic on that, but it avoided a huge amount of patient discomfort,” Professor Brazil says.
“Other examples are things that make healthcare professionals happier and more satisfied at work, which is particularly important at a time when workforce retention is so vital.
“One of my colleagues in Denmark has just demonstrated doing this kind of work reduces sick leave, which makes such a difference. If healthcare professionals are satisfied and fulfilled in their job, and feel the systems support them, that is priceless.”

A new partnership opens access
Professor Brazil says lowering the barriers to designing and delivering translational simulation is the next phase in opening access to more health services, from hospitals through to community care, and the individuals who work within them.
There is also huge opportunity to expand translational simulation to those who have never participated in simulation-based education before, such as those in quality improvement and patient safety units. But effective simulations are complex.
“You have got to think about the approach to identifying the real problem you are working on, and what kind of simulation design will work. Are you mocking up a cardboard cut-out of the resource room, or working with actors or mannequins? And then, how do you collect data out of the simulations to inform improvement?” Professor Brazil says.
It's led to a groundbreaking new industry partnership between Bond University and family-owned Norwegian firm Laerdal. It couples Bond’s expertise developed through work with institutions like Gold Coast University Hospital, Sydney Children's Hospital and Singapore’s Woodlands Hospital, with Laerdal’s six-decade record of developing tools to improve patient care.
It is taking translational simulation into the next frontier, harnessing artificial intelligence to improve accessibility and outcomes.
AI-powered translational simulation
The partnership is working on a new project, involving the design of a custom large language model (LLM) that provides bespoke recommendations drawn from credible referenced material and resources.
“It takes all that wisdom and steps you through the design phase to the delivery phase, to data collection and, ultimately, generating reports to inform improvement,” Professor Brazil says.
“You can upload documents in a safe, secure software platform. It is specific for this context and gives more precise answers because we have purpose created it.
“It is all very interesting for me. I’m not a software developer, so it has been impressive to see how much time it saves, as well as giving you tools and resources that might be outside your average simulation healthcare professionals’ knowledge and expertise.”
Global improvements
From its Gold Coast roots, translational simulation is being adopted globally. Bond’s Translational Simulation in Healthcare microcredential, introduced in 2023, has already helped hospitals throughout Australia, Singapore and the United Kingdom.
The new project with Laerdal will further extend the method’s global reach. Professor Brazil says while it is exciting, she is firmly focused on the on-the-ground positive impacts for patients and healthcare professionals.
“I know from my emergency medicine background the frustrations when systems don't work. So back to that basic premise, the idea we can do something that helps those people not have as frustrating a time is a really good feeling,” she says.
“The global reach is nice, but to me it is more important that we continue to refine the methodology as more people do it. It becomes clear what’s best practice and most helpful. We will continue to get better at the technique the more we do.”


Global improvements
From its Gold Coast roots, translational simulation is being adopted globally. Bond’s Translational Simulation in Healthcare microcredential, introduced in 2023, has already helped hospitals throughout Australia, Singapore and the United Kingdom.
The new project with Laerdal will further extend the method’s global reach. Professor Brazil says while it is exciting, she is firmly focused on the on-the-ground positive impacts for patients and healthcare professionals.
“I know from my emergency medicine background the frustrations when systems don't work. So back to that basic premise, the idea we can do something that helps those people not have as frustrating a time is a really good feeling,” she says.
“The global reach is nice, but to me it is more important that we continue to refine the methodology as more people do it. It becomes clear what’s best practice and most helpful. We will continue to get better at the technique the more we do.”

Original thinking direct to your inbox

Stories from Bond